Akanthose
| Klassifikation nach ICD-10 | |
|---|---|
| L85 | Sonstige Epidermisverdickung (und je nach Krankheitsbild) |
| ICD-10 online (WHO-Version 2019) | |
Die Akanthose (griechisch akanthos „dornig“, „stachelig“) bezeichnet in der Medizin eine Verbreiterung der Stachelzellschicht (Stratum spinosum)[1] des Plattenepithels (spezialisierte oberflächliche Zellschicht) der Oberhaut (Epidermis) und bestimmter Schleimhäute durch Vermehrung oder Vergrößerung der Zellen. Oft stellt sie eine Regenerationsreaktion auf mechanische Belastung oder Entzündungen[2] dar und tritt dann ggf. zusammen mit einer gestörten Verhornung (Hyper- oder Parakeratose) auf. Sie kann aber auch genetisch bedingt, im Rahmen bestimmter Grunderkrankungen oder als Nebenwirkung von Medikamenten[3] auftreten. Je nach Ursache zeigt sich ein unterschiedliches klinisches Bild mit umschriebener Verdickung der Haut. Das verbreiterte Stratum spinosum ist nur unter dem Mikroskop (histologisch) sichtbar.
 Epidermis, schematisch
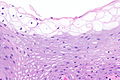
Epidermis, schematisch normale Haut, histologisch
normale Haut, histologisch
Entstehung
Durch Hyperplasie (Zunahme der Zellzahl) und/oder Hypertrophie (Zellvergrößerung) der Keratinozyten (flache Zellen des Plattenpithels) kommt es zur Verbreiterung des Stratum spinosum und somit des gesamten Epithels. Die Zunahme der Zellzahl kann Resultat einer vermehrten Teilung von Reservezellen (auch: Basalzellen, Proliferationsakanthose) oder einer verzögerten Ausreifung der Keratinozyten (Zellen des Plattenepithels) sein (Retentionsakanthose).[4] Durch eine Verlängerung der Retezapfen (Verzahnung des Epithels mit dem unterliegenden Bindegewebe) kann außerdem die Fläche der teilungsaktiven Reservezellschicht (Stratum basale) vergrößert werden.[5]
Klinische Erscheinung
Je nach Ursache der Akanthose kommt es durch die Verdickung der Epidermis zur Ausbildung von Papeln, Knötchen oder ausgedehnten Plaques, die gerötet (durch Entzündung), weißlich (durch vermehrte und/oder gestörte Verhornung oder Speicherung von Glykogen) oder braun (durch verstärkte Pigmentierung) erscheinen können.
Vorkommen
Im Rahmen von entzündlichen Hauterkrankungen tritt eine Akanthose klassischerweise bei der Psoriasis (Schuppenflechte) auf, bei der sie mit einer deutlichen Verlängerung der Retezapfen einhergeht (psoriasiforme Akanthose). Sie ist aber z. B. auch bei länger bestehenden Ekzemerkrankungen, dem Lichen ruber planus und Insektenstichen zu beobachten.
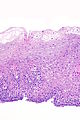
 Psoriasis, histologisch: typische Akanthose mit ausgezogenen Retezapfen
Psoriasis, histologisch: typische Akanthose mit ausgezogenen Retezapfen Psoriasis, klinisch
Psoriasis, klinisch
Bestimmte nicht-entzündliche Hautveränderungen und gutartige Tumoren der Epidermis wie z. B. Alters-[6] oder Viruswarzen[7] gehen ebenfalls mit einer stark lokal begrenzten Akanthose einher, sie werden deshalb auch als Akanthome bezeichnet.
 Alterswarze, histologisch
Alterswarze, histologisch Alterswarze, klinisch
Alterswarze, klinisch Viruswarze, histologisch
Viruswarze, histologisch Viruswarze, klinisch
Viruswarze, klinisch
Als Acanthosis nigricans werden flächige Manifestationen einer Akanthose bezeichnet, die erblich als familiäre Acanthosis nigricans oder im Rahmen genetischer Syndrome (z. B. Alström-[8] oder Crouzon-Syndrom[9]), mit verschiedenen Grunderkrankungen (z. B. bösartige Tumorerkrankungen[10], Diabetes mellitus[11], Lupus erythematodes[12]) oder nach Medikamenteneinnahme (z. B. Nikotinsäure[13]) auftreten[14].
 familiäre Acanthosis nigricans, klinisch
familiäre Acanthosis nigricans, klinisch Acanthosis nigricans, klinisch
Acanthosis nigricans, klinisch
An der Schleimhaut der Speiseröhre kann es durch Einlagerung von Glykogen in den Keratinozyten zu einer Glykogenakanthose kommen, die möglicherweise Folge einer Refluxerkrankung (Sodbrennen) darstellt[15].
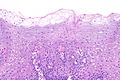
 Glykogenakanthose des Ösophagus, histologisch
Glykogenakanthose des Ösophagus, histologisch

An Körperstellen mit hoher mechanischer Belastung wie Handflächen und Fußsohlen zeigt sich naturgemäß dickere Haut mit langen Retezapfen, um eine angemessene Regeneration des Epithels zu ermöglichen[16].
 mechanisch beanspruchte Haut, histologisch: dicke Epidermis mit langen Retezapfen
mechanisch beanspruchte Haut, histologisch: dicke Epidermis mit langen Retezapfen Fingerspitze, OCT: Haut mit langen Retezapfen
Fingerspitze, OCT: Haut mit langen Retezapfen
Einzelnachweise
- ↑ Otto Braun-Falco, Gerd Plewig, Helmut H. Wolff: Dermatologie und Venerologie. 3., neubearb. Auflage. Springer-Verlag, Berlin 1996, ISBN 978-3-540-12023-0, S. 14 (OCLC 612292746).
- ↑ W. Böcker: Pathologie. 4., vollst. überarb. Auflage. München 2008, ISBN 978-3-437-42382-6, S. 1027 f. (OCLC 723846189).
- ↑ Eduardo Calonje, Thomas Brenn, Alexander Lazar, Steven D. Billings: McKee’s pathology of the skin with clinical correlations. Fifth edition Auflage. Elsevier, ohne Ort 2020, ISBN 978-0-7020-7552-0, S. 626 ff. (OCLC1085350565).
- ↑ P. Altmeyer, M. Bacharach-Buhles: Akanthose. In: Altmeyers Enzyklopädie. Abgerufen am 10. April 2021.
- ↑ Max Eder, Heinz Bechtelsheimer: Allgemeine Pathologie und pathologische Anatomie. 33., neubearb. u. erw. Auflage. Berlin 1990, ISBN 3-540-51899-1, S. 784 (OCLC 246719725).
- ↑ Eduardo Calonje, Thomas Brenn, Alexander Lazar, Steven D. Billings: McKee’s pathology of the skin with clinical correlations. Fifth edition Auflage. Elsevier, ohne Ort 2020, ISBN 978-0-7020-7552-0, S. 1162 (OCLC 1085350565).
- ↑ Eduardo Calonje, Thomas Brenn, Alexander Lazar, Steven D. Billings: McKee’s pathology of the skin with clinical correlations. Fifth edition Auflage. Elsevier, ohne Ort 2020, ISBN 978-0-7020-7552-0, S. 829 (OCLC 1085350565).
- ↑ K. W. Chang, J. W. Hou, S. J. Lin, M. S. Kong: Alstrom syndrome with hepatic dysfunction: report of one case. In: Acta Paediatrica Taiwanica = Taiwan Er Ke Yi Xue Hui Za Zhi. Band 41, Nr. 5, 2000, ISSN 1608-8115, S. 270–272, PMID 11100527.
- ↑ T. Nagase, M. Nagase, S. Hirose, K. Ohmori: Crouzon syndrome with acanthosis nigricans: case report and mutational analysis. In: The Cleft Palate-Craniofacial Journal: Official Publication of the American Cleft Palate-Craniofacial Association. Band 37, Nr. 1, Januar 2000, ISSN 1055-6656, S. 78–82, doi:10.1597/1545-1569_2000_037_0078_cswanc_2.3.co_2, PMID 10670894.
- ↑ Mirella Krawczyk, Joanna Mykała-Cieśla, Aleksandra Kołodziej-Jaskuła: Acanthosis nigricans as a paraneoplastic syndrome. Case reports and review of literature. In: Polskie Archiwum Medycyny Wewnetrznej. Band 119, Nr. 3, März 2009, S. 180–183, PMID 19514649.
- ↑ Eduardo Calonje, Thomas Brenn, Alexander Lazar, Steven D. Billings: McKee’s pathology of the skin with clinical correlations. Fifth edition Auflage. Elsevier, ohne Ort 2020, ISBN 978-0-7020-7552-0, S. 628 (OCLC 1085350565).
- ↑ J. S. Baird, J. L. Johnson, D. Elliott-Mills, L. M. Opas: Systemic lupus erythematosus with acanthosis nigricans, hyperpigmentation, and insulin receptor antibody. In: Lupus. Band 6, Nr. 3, 1997, ISSN 0961-2033, S. 275–278, doi:10.1177/096120339700600311, PMID 9104736.
- ↑ H. Stals, C. Vercammen, C. Peeters, M. A. Morren: Acanthosis nigricans caused by nicotinic acid: case report and review of the literature. In: Dermatology. Band 189, Nr. 2, 1994, ISSN 1018-8665, S. 203–206, doi:10.1159/000246834, PMID 8075456.
- ↑ Eduardo Calonje, Thomas Brenn, Alexander Lazar, Steven D. Billings: McKee’s pathology of the skin with clinical correlations. Fifth edition Auflage. Elsevier, ohne Ort 2020, ISBN 978-0-7020-7552-0, S. 626 ff. (OCLC1085350565).
- ↑ M. Vieth, C. Langner, J. Rüschoff: Pathologie - Verdauungstrakt und Peritoneum. In: G. Klöppel, H. H. Kreipe, W. Remmele (Hrsg.): Pathologie. 3., neubearbeitete Auflage. Springer, Berlin 2013, ISBN 978-3-642-02322-4, S. 37 (OCLC 849918529).
- ↑ Gordon I. Kaye, Wojciech Pawlina: Histology: a text and atlas. 4. Auflage. Lippincott Williams & Wilkins, Philadelphia PA 2003, ISBN 0-683-30242-6, S. 404 (OCLC 50334073 [abgerufen am 12. April 2021]).
Auf dieser Seite verwendete Medien

Autor/Urheber: Jenny Giang, Marc A. J. Seelen, Martijn B. A. van Doorn, Robert Rissmann,Errol P. Prens and Jeffrey Damman, Lizenz: CC BY 4.0
Micrograph of psoriasis vulgaris. Confluent parakeratosis, psoriasiform epidermal hyperplasia [(A), EH], hypogranulosis, and influx of numerous neutrophils in the corneal layer [(A), arrow]. (B) Transepidermal migration of neutrophils from the dermis to the corneal layer (arrows).
Autor/Urheber: Nephron, Lizenz: CC BY-SA 3.0
Micrograph showing acanthosis and superficial clearing of the esophagus', also known as glycogenic acanthosis of the eosphagus (abbreviated GAE). H&E stain.
Related images
-
 GAE - low mag.
GAE - low mag. -
 GAE - intermed. mag.
GAE - intermed. mag. -
 GAE - intermed. mag.
GAE - intermed. mag. -
 GAE - high mag.
GAE - high mag. -
 GAE - very high mag.
GAE - very high mag. -
 GAE - intermed. mag.
GAE - intermed. mag. -
 GAE - high mag.
GAE - high mag.








Diagram of the layers of the epithelial skin layer: the epidermis.


Autor/Urheber: User:BoP, Supplied by the medOCT group, Medical University Vienna, Austria, Lizenz: CC BY-SA 2.0 at
Rotating image of Optical Coherence Tomography (OCT) tomogram of a fingertip, depicting stratum corneum (~500µm thick) with stratum disjunctum on top and stratum lucidum (connection to stratum spinosum) in the middle. At the bottom are superficial parts of the dermis. Sweatducts are clearly visible. This animated image loads 85x times slower than the non-animated image.

Autor/Urheber: Nephron, Lizenz: CC BY-SA 3.0
Very low magnification micrograph of a verruca vulgaris, a common wart. H&E stain.
Features:
- Hyperkeratosis.
- Acanthosis.
- Hypergranulosis.
- Long rete ridges.
- Large blood vessels at the dermal-epidermal junction.
Related images
-
 Very low mag.
Very low mag. -
 Low mag.
Low mag. -
 Intermed. mag.
Intermed. mag. -
 High mag.
High mag.





Autor/Urheber: Mikael Häggström, based on work by Wbensmith, Lizenz: CC BY-SA 3.0
Layers of the epidermis

Autor/Urheber: Vandana Mehta Rai MD DNB, C Balachandran MD, Lizenz: CC BY-SA 3.0
en:Familial acanthosis nigricans, 13-year-old boy with an 8-year history of generalized hyperpigmentation and velvety thickening of the skin. Based on the history and clinical examination a diagnosis of benign AN was considered. The diagnosis of epidermolytic hyperkeratosis was considered, but was excluded on the basis of negative history and histopathological findings. The patient was treated with oral vitamin A , topical retinoids, and keratolytics. After follow up for one year neither endocrinological nor malignant diseases have developed. source

Autor/Urheber: Nephron, Lizenz: CC BY-SA 3.0
Intermediate magnification micrograph of a seborrheic keratosis. H&E stain.
Related images
-
 Low mag.
Low mag. -
 Intermed. mag.
Intermed. mag. -
 High mag.
High mag.





Autor/Urheber: Mark F. Brady; Prashanth Rawla., Lizenz: CC BY-SA 4.0
Acanthosis nigricans on axilla


This is a hematoxylin and eosin stained slide at 10x of normal epidermis and dermis with a benign intradermal nevus. (Cropped to show only the epidermis.)